
Ferritin levels in pregnancy chart—do you know why tracking this iron-storage protein matters so much? Ferritin reflects the amount of iron your body keeps in reserve, which becomes critical when supporting a developing baby. Wondering what normal ferritin ranges look like during each stage of pregnancy? Let’s break it down clearly.
Typically, ferritin levels should stay between 30–200 ng/mL before pregnancy, but they often dip to around 15–60 ng/mL by the third trimester. This drop happens as your body transfers iron to the growing fetus and expands blood volume. According to Dr. Mary E. D’Alton, a leading maternal-fetal medicine specialist, monitoring ferritin alongside hemoglobin helps clinicians detect early iron deficiency before anemia sets in.
Monitoring iron stores across pregnancy is crucial, and many obstetric clinicians and researchers refer to a Iron Levels in Pregnancy Chart to track typical values by trimester, detect iron deficiency early, and optimize maternal-fetal health.
Curious to see how these numbers change across all three trimesters and what they mean for your health? In the main article, you’ll find a trimester-wise ferritin chart and expert tips to maintain healthy iron stores. Let’s explore the data and learn how to protect both mother and baby with timely iron management.
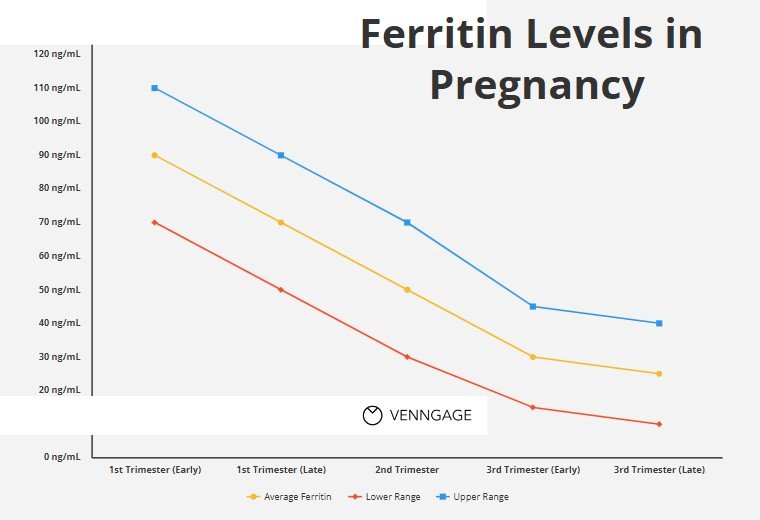
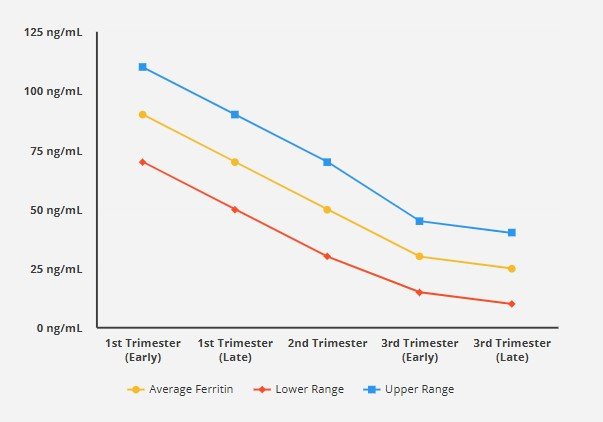
Ferritin Levels in Pregnancy Chart (Trimester-By-Trimester)
Below is a representative Ferritin Levels in Pregnancy Chart (trimester-by-trimester), based on physiologically derived thresholds and literature synthesis:
| Trimester | Approximate Ferritin Threshold (μg/L) | Clinical Interpretation* |
|---|---|---|
| First trimester | ~ 25.8 μg/L (≈ 25 μg/L) | Below this: likely early iron depletion / deficiency |
| Second trimester | ~ 18.3 μg/L (≈ 20 μg/L) | Below: risk of iron-deficient state |
| Third trimester | ~ 19.0 μg/L (≈ 20 μg/L) | Persistently low: risk of iron deficiency anemia |
| Alternative conservative cutoff† | 15 μg/L (all trimesters) | Traditional “iron deficiency” threshold (WHO/CDC) |
* These thresholds are based on physiological modeling bridging hemoglobin (Hb) and soluble transferrin receptor (sTfR) behavior.
† WHO and CDC guidelines often use a ferritin < 15 μg/L cutoff, though that may underestimate deficiency in pregnancy.
Interpretation & caveats:
- These values are thresholds, not “normal ranges” per se. In early pregnancy, higher ferritin is acceptable; in later trimesters, values decline due to physiological demands.
- Ferritin is an acute-phase reactant: it may be falsely elevated in inflammation, infection, or other stress states, masking true deficiency.
- These trimester-specific thresholds are relatively new and not universally adopted; many labs and clinicians still rely on older cutoffs (e.g. < 15 μg/L).
Clinically, if a patient’s ferritin falls substantially below these thresholds (especially when combined with low hemoglobin), it raises the possibility of iron deficiency and merits further evaluation or supplementation (depending on severity).
Reference Values For Ferritin Pregnancy
When discussing “reference values” for ferritin in pregnancy, it is critical to distinguish between statistical reference intervals (i.e. what is observed in a healthy cohort) and functional or clinical cutoffs (i.e. thresholds for deficiency or intervention). For ferritin in pregnancy, literature and guidelines show significant variability.
Traditional / guideline cutoffs
- The World Health Organization (WHO) has long considered a ferritin < 15 µg/L as indicative of iron deficiency in pregnancy, particularly in the first trimester. pmc.ncbi.nlm.nih.gov+2ashpublications.org+2
- The CDC similarly often uses ≤ 15 µg/L across trimesters. ashpublications.org+1
- Some clinical protocols (e.g. Alberta Health Services) use a more generous threshold, flagging ferritin < 30 µg/L in pregnant patients as a reason for concern or intervention. Alberta Health Services
- In broader adult (non-pregnant women), typical ferritin reference ranges are ~ 15–200 ng/mL (or µg/L) depending on lab method. Cleveland Clinic+2urmc.rochester.edu+2
Physiologically based trimester-adjusted thresholds
A more recent and sophisticated method seeks to align ferritin cutoffs with the physiologic changes of pregnancy. One study using cross-sectional NHANES data employed regression spline modeling of hemoglobin (Hb) and soluble transferrin receptor (sTfR) vs. ferritin, defining “breakpoints” (plateaus) that suggest minimal iron sufficiency during each trimester. pmc.ncbi.nlm.nih.gov Their findings:
- First trimester: ~ 25.8 µg/L
- Second trimester: ~ 18.3 µg/L
- Third trimester: ~ 19.0 µg/L
These thresholds are higher than WHO/CDC standards and may identify more women with early iron deficiency before hemoglobin falls.
Observational cohort findings
- In a study of pregnant women at term, mean ferritin was ~ 47.8 µg/L (± 98.4) in a cohort that largely received iron supplementation during pregnancy. pmc.ncbi.nlm.nih.gov
- Another study observed that serum ferritin concentrations in early pregnancy in healthy pregnant women often fall within broad ranges, with the 75th percentile around 45 µg/L. pmc.ncbi.nlm.nih.gov
- Some research establishes “normal reference” serum ferritin in pregnant women as 13–150 µg/L, acknowledging wide interindividual variation. Nature
Practical considerations & limitations
- Because ferritin reflects both iron stores and systemic inflammation, elevated ferritin does not always mean iron sufficiency; conversely, low ferritin in the presence of inflammation may underestimate deficiency.
- Many laboratories do not generate pregnancy-specific reference ranges, so clinicians must interpret pregnant ferritin values in light of physiology and risk factors (e.g. anemia, diet, bleeding).
- There is no universal consensus yet to adopt the newer physiologically derived thresholds; many guidelines continue using < 15 µg/L for deficiency. pmc.ncbi.nlm.nih.gov+2ashpublications.org+2
In sum, rather than rigidly adhering to a single “normal” range, it is more clinically powerful to use trimester-adjusted threshold values (as in the chart above) together with hemoglobin, red cell indices, and clinical features to diagnose and manage iron deficiency in pregnancy.
Hematological Normal Ranges in Pregnancy
Assessing ferritin in pregnancy must be contextualized within the broader hematologic changes that occur during gestation. Pregnancy induces profound physiological shifts in blood volume, red cell mass, and hemodilution.
Here’s a concise yet comprehensive overview of hematologic norms during pregnancy and how they relate to ferritin interpretation.
Hemodynamic and hematologic adaptation in pregnancy
- Plasma volume expands by approximately 40–50%, whereas red cell mass increases by only 20–30%, causing a dilutional (physiologic) drop in hemoglobin and hematocrit (the so-called “physiologic anemia”). en.wikipedia.org+1
- Erythropoietin production increases, and iron absorption adjusts to meet increased demands. ashpublications.org+1
- The nadir of hemoglobin and hematocrit typically occurs in the late second trimester (around 28–32 weeks). ashpublications.org+2glowm.com+2
- Toward term, mild hemoconcentration may restore hemoglobin slightly. ashpublications.org+1
Trimester-specific hemoglobin / anemia cutoffs
The WHO and many obstetric guidelines define anemia in pregnancy by trimester-adjusted hemoglobin (Hb) levels:
- First trimester: Hb < 11.0 g/dL (anemia) ashpublications.org+2ashpublications.org+2
- Second trimester: Hb < 10.5 g/dL ashpublications.org+2ashpublications.org+2
- Third trimester: Hb < 11.0 g/dL ashpublications.org+2ashpublications.org+2
These cutoffs correspond to the physiological hemodilution pattern. ashpublications.org+2glowm.com+2
Normal ranges for other red cell indices in pregnancy
- Hematocrit (Hct): Because of hemodilution, hematocrit reference ranges shift downward; typical values in pregnancy are ~ 32–36% (varies by lab). glowm.com+2Alberta Health Services+2
- Mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH): These indices are generally stable; microcytosis or low MCV raises suspicion of iron deficiency. glowm.com
- Red cell distribution width (RDW): May widen in early iron deficiency; not uniquely pregnancy modified. glowm.com
- Reticulocyte count: Increased reticulocytes may reflect compensatory erythropoiesis, but normal reference ranges are somewhat preserved. glowm.com
- White blood cell (WBC) count: Mild leukocytosis during pregnancy is common; upper normal values may exceed nonpregnant women limits. glowm.com+1
- Platelet count: Slight decline in platelet count (gestational thrombocytopenia) is common; moderate declines are within normal variation. glowm.com+1
How ferritin fits into the hematologic picture
- Ferritin provides an indirect measure of iron stores, complementing red cell indices and hemoglobin.
- In early pregnancy when hemodilution is minimal, a higher ferritin is expected; later in pregnancy, lower ferritin is normal if iron stores are being drawn down.
- Declining hemoglobin with a low ferritin suggests iron deficiency anemia (IDA); declining hemoglobin with normal/high ferritin may suggest alternate causes (e.g. anemia of inflammation, hemolysis, B12/folate deficiency).
- Because ferritin is influenced by inflammation, it’s clinically prudent to evaluate C-reactive protein (CRP) or alpha-1-acid glycoprotein (AGP) when interpreting borderline ferritin values.
In summary, interpreting ferritin levels in pregnancy requires a holistic view of hematologic adaptation. A ferritin test is most meaningful when considered alongside hemoglobin, red cell indices, reticulocyte response, and inflammatory markers.
FAQs – about Iron Levels in Pregnancy Chart Third Trimesterof Pregnancy
What are ferritin levels and why are they important during pregnancy?
Ferritin levels indicate the amount of stored iron in the body, which is crucial for pregnant women to ensure adequate iron supply for both maternal health and fetal development. Low ferritin levels can signal iron deficiency anemia, which can lead to complications during pregnancy.
How do ferritin levels change throughout pregnancy?
Ferritin levels typically fluctuate during pregnancy, often decreasing in the first and second trimesters due to increased blood volume and iron demands. By the third trimester, ferritin levels may stabilize or further decline if iron supplementation is not adequately addressed.
What are the thresholds for iron deficiency in pregnant women?
The World Health Organization recommends specific thresholds for ferritin levels to diagnose iron deficiency anemia in pregnancy. Generally, a ferritin level below 30 ng/mL is considered indicative of iron deficiency, while levels below 15 ng/mL suggest iron deficiency anemia.
What is the prevalence of anemia in pregnancy?
The prevalence of anemia in pregnancy varies by population but is generally higher in developing countries. Studies indicate that a significant percentage of healthy women during pregnancy may experience iron deficiency anemia, necessitating screening for anemia and iron deficiency, particularly in the second and third trimesters.
What are the common causes of iron deficiency anemia in pregnancy?
Common causes include inadequate dietary iron intake, increased iron demands due to fetal growth, and blood loss during delivery. Pregnant women may also have lower iron stores if they had pre-existing deficiencies before conception.
How can pregnant women improve their ferritin levels?
Pregnant women can improve their ferritin levels through dietary changes, such as consuming iron-rich foods, and taking iron supplements, including oral iron or intravenous iron, depending on their specific needs and physician recommendations.
What role do iron supplements play in managing ferritin levels?
Iron supplements are critical for maintaining healthy ferritin levels in pregnant women, especially if they have been diagnosed with iron deficiency anemia. Oral iron is commonly used, but intravenous iron may be necessary for those who cannot tolerate oral forms or have severe deficiencies.
How is the diagnosis of iron deficiency made during pregnancy?
The diagnosis of iron deficiency in pregnancy typically involves blood tests to measure serum ferritin, serum iron, transferrin levels, and total iron-binding capacity. A comprehensive assessment helps determine the appropriate treatment and monitoring plan.
What are the implications of low ferritin levels for maternal and fetal health?
Low ferritin levels can lead to an increased risk of complications such as preterm birth, low birth weight, and postpartum hemorrhage. For the fetus, inadequate iron can impact cognitive and physical development, highlighting the importance of maintaining optimal iron status throughout pregnancy.
Are there any risks associated with iron supplementation during pregnancy?
While iron supplementation is generally safe, excessive intake can lead to side effects such as gastrointestinal discomfort or constipation. It’s crucial for pregnant women to follow healthcare provider recommendations regarding dosage to avoid potential complications.
What is the recommended approach to screening for iron deficiency in pregnant women?
Screening for iron deficiency should begin early in pregnancy, with follow-up evaluations in the second and third trimesters. Regular monitoring of ferritin levels, along with clinical assessments, helps ensure timely intervention and management of iron status.
Conclusion
Understanding and applying a Ferritin Levels in Pregnancy Chart (trimester-by-trimester) offers clinicians and pregnant women a more nuanced lens to assess iron status than rigid, one-size-fits-all cutoffs. The physiologically derived thresholds (~ 25 µg/L in the first trimester, ~ 18–20 µg/L in the second and third) help identify early iron deficiency before frank anemia develops. These thresholds are superior to the traditional < 15 µg/L standard in detecting more subtle deficiencies, especially as pregnancy progresses. pmc.ncbi.nlm.nih.gov
Still, ferritin interpretation must be contextual: laboratory variability, inflammatory states, and individual physiology all influence values. By combining trimester-specific ferritin thresholds with hemoglobin cutoffs, red cell indices, reticulocyte response, and clinical context, clinicians can more accurately stratify risk, tailor iron therapy, and ultimately support better maternal and fetal outcomes.
Recommended posts
- The Physiology of Anemia in Pregnancy in Expecting Mothers
- How to Increase Hemoglobin in Pregnancy (5 Proven Ways)
- Top 10 Foods High in Iron for Pregnancy – You Should Eat
- What to Drink to Increase Hemoglobin? (Iron Rich Drinks List)
- Is Iron Infusions in Pregnancy Safe? (Essential Guide)
- High WBC in Pregnancy: Causes, Normal Ranges, and Concerns

