
Did you know that there are 4 types of Placenta Previa that can affect a pregnancy? This condition, where the placenta blocks or partially covers the cervix, often raises concern among expecting mothers. But what exactly are these types, and how do they differ in risks and treatment options?
The four placenta previa types are Complete Placenta Previa, Partial Placenta Previa, Marginal Placenta Previa, and Low-Lying Placenta. Each type varies in terms of how much the placenta covers the cervix and how it may impact delivery. Obstetrics and gynecology like Dr. Robert Resnik, a leading authority in maternal-fetal medicine, emphasize that recognizing these distinctions is crucial for safe pregnancy care.
Curious to know how each type affects pregnancy outcomes and what expert advice says about managing them? You’ll find a clear breakdown of the four types, along with trusted medical insights that make complex details easy to grasp. So, let’s dive into the details and explore everything you need to know about Placenta Previa.
What Causes Placenta Previa?
The exact cause of placenta previa isn’t always clear, but medical research has identified several significant risk factors that increase the likelihood of the placenta implanting low in the uterus.
It’s important to understand that in many early pregnancies, a low-lying placenta is common. However, as the uterus grows and stretches, the placenta typically migrates upward and away from the cervix—a process known as “placental migration.” Placenta previa is diagnosed when this migration does not occur by the third trimester.
The primary risk factors associated with placenta previa include:
- Previous Uterine Surgery: This is one of the most prominent risk factors. Any procedure that creates scarring on the uterine lining (the endometrium) can affect where a fertilized egg implants. This includes previous Cesarean deliveries (C-sections), surgical removal of fibroids (myomectomy), or a D&C (dilation and curettage) procedure.
- Multiple Pregnancies: Women carrying multiples (twins, triplets, etc.) have a larger placental area, which statistically increases the chance of the placenta covering or nearing the cervix.
- Advanced Maternal Age: Pregnancies in women over the age of 35 are associated with a higher incidence of placenta previa.
- High Number of Previous Pregnancies: Having had several previous pregnancies increases the risk.
- Smoking and Substance Use: Tobacco use and cocaine use have been strongly linked to an increased risk of placenta previa, as these substances can affect the implantation of the placenta.
- History of Placenta Previa: A woman who has had placenta previa in a previous pregnancy is at a higher risk of experiencing it again.
- In Vitro Fertilization (IVF): Pregnancies achieved through IVF have a slightly higher associated risk of placenta previa.
The 4 Types of Placenta Previa – Shouldn’t Ignore
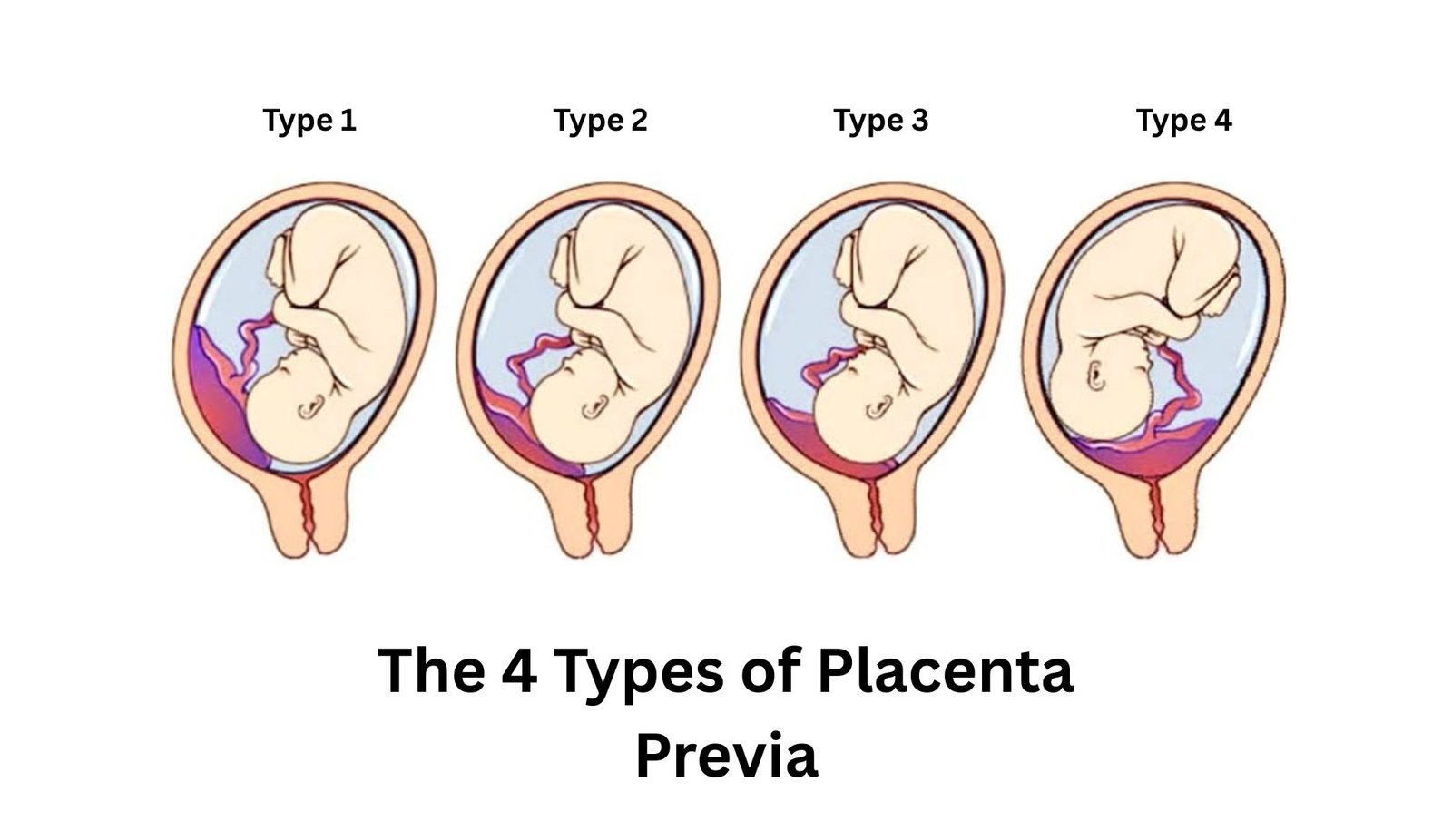
The classification of placental previa is determined by how much the placenta covers the internal opening of the cervix, as visualized during a transvaginal ultrasound. This precise classification is critical for your obstetrician to develop a safe delivery plan. The four types are generally categorized as follows, moving from least to most severe.
1. Low-lying Placenta
In this type, the placenta implants in the lower segment of the uterus but does not reach the border of the cervical opening (the internal os). It is in close proximity but not covering it. This is often the mildest form, and because the edge of the placenta is not covering the exit, a vaginal delivery may sometimes still be possible if sufficient distance is maintained as the pregnancy progresses.
2. Marginal Placenta Previa
Also known as a grade I previa, the marginal type occurs when the edge of the placenta extends to the very border of the cervical opening but does not cover it. Think of it as the placenta “touching the finish line” but not crossing it. While the potential for bleeding exists, the management may be similar to a low-lying placenta, with a chance of vaginal delivery if the distance is adequate.
3. Partial Placenta Previa (Grade II)
This type is more serious. As the name suggests, the placenta partially covers the internal cervical os. When the cervix begins to dilate, even slightly, a portion of the placenta is obstructing the birth canal, which will inevitably cause severe, painless bleeding. A partial placenta previa absolutely necessitates a cesarean delivery to prevent catastrophic hemorrhage during labor.
4. Complete or Total Placenta Previa (Grade III/IV)
This is the most severe type of placental previa. Here, the placenta completely covers the internal cervical os, forming a total blanket over the birth canal. Any attempt at cervical dilation or labor would cause the placenta to tear away, leading to life-threatening bleeding for both the mother and the baby. A planned C-section is the only safe delivery option, often scheduled several weeks before the due date to avoid the onset of natural labor.
A crucial note: The diagnosis can change as your pregnancy advances. A low-lying or marginal placenta previa identified at the 20-week anatomy scan often resolves on its own by 28-32 weeks as the uterus expands. Complete and partial previas are less likely to resolve.
What are the Signs and Symptoms of Placenta Previa?
The hallmark symptom of placenta previa is sudden, painless, bright red vaginal bleeding during the second or third trimester, most commonly after the 28th week. This bleeding is not associated with abdominal pain or contractions, which helps distinguish it from other conditions like placental abruption.
Other key signs and symptoms include:
- Recurrent Episodes: Bleeding from placenta previa often starts and stops, with episodes recurring days or weeks later.
- Uterine Cramping: While the bleeding is typically painless, some women may experience accompanying cramping or contractions, especially if bleeding is significant.
- The “Warning Gush”: The initial bleed can range from light spotting to a heavy flow. It often occurs without warning, sometimes during rest or sleep.
- Abnormal Fetal Positioning: Because the placenta is occupying space in the lower uterus, the baby may be in a breech (feet-first) or transverse (sideways) position.
Important: Any instance of vaginal bleeding during pregnancy warrants an immediate call to your healthcare provider or a trip to the emergency room. Do not ignore it. Diagnosis is confirmed via ultrasound, most accurately with a transvaginal probe.
Maternal Complications of Placenta Previa:
While modern obstetric care has dramatically improved outcomes, placenta previa remains a serious condition with potential risks for both the mother and the fetus. Understanding these complications underscores the importance of strict medical supervision.
For the Mother:
- Hemorrhage and Shock: The primary risk is severe, life-threatening bleeding (hemorrhage) before, during, or even after delivery, which can lead to shock and require blood transfusions.
- Placenta Accreta Spectrum (PAS): This is a serious complication where the placenta attaches too deeply into the uterine wall and does not separate properly after delivery. The risk of PAS is significantly higher in women with placental previa and a history of prior C-sections. It can lead to massive hemorrhage and often requires a hysterectomy (surgical removal of the uterus) to control bleeding.
- Preterm Birth: To avoid an emergency situation caused by a sudden bleed, an early planned C-section is often necessary, leading to a premature delivery.
- Emergency Surgery: An unexpected severe bleed can force an emergency cesarean delivery, which carries higher risks than a planned procedure.
- Blood Transfusion Risks: The need for a blood transfusion, while life-saving, carries its own small risks, including reactions and infection.
For the Baby:
- Preterm Birth: The most common complication for the baby is being born prematurely due to an early scheduled delivery or an emergency caused by maternal bleeding. This can lead to respiratory distress syndrome, low birth weight, and other challenges associated with prematurity.
- Fetal Growth Restriction: Significant bleeding can sometimes compromise the placenta’s function, potentially affecting the baby’s oxygen and nutrient supply.
- Fetal Anemia: In rare cases of severe bleeding, the baby can lose blood, leading to anemia.
Management involves close monitoring, pelvic rest (no intercourse or tampons), and potentially hospitalization and steroid injections to accelerate the baby’s lung development in case of an early delivery.
Commonly Asked Questions about Types of Placenta Praevia (FAQs)
What is the difference between placenta previa and placental abruption?
Placenta previa involves the placenta covering the cervix, causing painless bleeding. Placental abruption is premature separation from the uterus, causing painful bleeding and fetal distress. Both are serious but distinct conditions.
How is placenta previa diagnosed?
Placenta previa is diagnosed via ultrasound, typically during the 20-week anatomy scan. Transvaginal ultrasound may be used for greater accuracy to confirm placental position relative to the cervix.
Can I have placenta previa without bleeding?
Yes, you can have placenta previa without bleeding, but it carries a high risk of bleeding if the blood vessels near the cervix are disturbed. Your medical history and ultrasound determine monitoring needs.
When should I see my healthcare provider?
See your healthcare provider for routine check-ups, persistent symptoms, or sudden changes in health. Seek immediate care for severe pain, heavy bleeding, high fever, or any urgent concerns about your or your baby’s well-being.
What is the vasa previa?
Vasa previa is a rare condition where fetal blood vessels run unprotected across the cervical opening. If ruptured during labor, it causes rapid fetal hemorrhage, requiring urgent cesarean delivery for survival.
What is placenta previa and how does it occur?
Placenta previa is a condition that occurs when the placenta is positioned low in the uterus, covering the cervix. This can lead to complications during pregnancy and delivery. The exact cause is not always clear, but factors such as previous surgeries, multiple pregnancies, and advanced maternal age may contribute to the condition. It is classified into four types based on the location of the placenta: complete, partial, marginal, and low-lying placenta previa.
How is placenta previa diagnosed during pregnancy?
To diagnose placenta previa, healthcare providers typically use a vaginal ultrasound, which allows them to visualize the location of the placenta in relation to the cervix. This is often done during routine check-ups, especially if there is a history of bleeding or other risk factors. Diagnosis is usually confirmed around 20 weeks of gestation, but the position of the placenta may change as the pregnancy progresses.
What are the common symptoms of placenta previa?
A common symptom of placenta previa is vaginal bleeding, particularly in the second half of pregnancy. This bleeding can occur without pain, making it crucial for expectant mothers to seek medical attention if they experience any unusual bleeding. Other symptoms may include uterine contractions or pressure in the lower uterine segment. It’s essential for women diagnosed with this condition to monitor their symptoms closely.
What are the risks associated with placenta previa?
The greatest risk of placenta previa is significant bleeding, which can pose serious health concerns for both the mother and the baby. If the placenta is covering the cervix, vaginal delivery may not be safe, and a cesarean section may be necessary. Additionally, the prevalence of placenta previa is around 1 in 200 pregnancies, and women with this condition may experience complications such as low blood pressure or premature birth.
Can the position of the placenta change during pregnancy?
Yes, the position of the placenta can change as the pregnancy progresses. In many cases of placenta previa, a low-lying placenta may move upward as the uterus expands, decreasing the chances of complications. However, some women may develop true placenta previa, where the placenta remains over the cervix. Regular check-ups and ultrasounds are essential to monitor the location of the placenta and determine the best course of action as gestational age increases.
Conclusion
A diagnosis of placenta previa can understandably be a source of significant anxiety for any expecting mother. However, armed with knowledge and under the expert care of a medical team, it is a highly manageable condition. The critical takeaways are to recognize the 4 types of placenta previa, understand that the key symptom is painless vaginal bleeding requiring immediate medical attention, and adhere strictly to your doctor’s recommendations.
Modern obstetrics is exceptionally well-equipped to handle this complication through careful monitoring, planned delivery via cesarean section, and preparedness for potential blood loss. By attending all prenatal appointments and following medical guidance, you are taking the most powerful steps to ensure the safest possible outcome for you and your precious baby.
Related posts
- Chances of Placenta Previa Moving After 32 Weeks (Revealed)
- Nursing Diagnosis for Placenta Previa: (Best Care Plan)
- What Is Low Lying Placenta? Causes, Risks & What to Expect
- Is Placenta Previa C Section Surgery Necessary?

